Calcific tendonitis is a form of tendinitis, a condition characterized by deposits of calcium in any tendon of the body, but most commonly in the tendons of the rotator cuff(shoulder), specially the supraspinatus causing pain and inflammation.
Calcific tendonitis can also be referred to as calcific tendinopathy, bone spurs in the tendon, calcium inside the tendon and others less common.
Calcific tendinopathy most often occurs in females aged 30 to 60 years and can occurs in 3–10% of the general population Calcifications are usually located within the supraspinatus tendon (80% of cases) which is the main tendon responsible for lifting the shoulder, followed by the infraspinatus (15% of cases) and subscapularis (5% of cases) tendons, but can be present in any tendon, and they are present in 5% or more of asymptomatic shoulders in healthy adults.
Signs and Symptoms
Around 50% of individuals with calcific tendinitis have symptoms. Symptoms include pain or weakness in the shoulder and often leads to decreased active range of motion.
Pain is often aggravated by elevation of the arm above shoulder level or by lying on the shoulder. Pain may awaken the patient from sleep. Other complaints may be stiffness, snapping, catching, or weakness of the shoulder.
How to diagnose calcific tendonitis
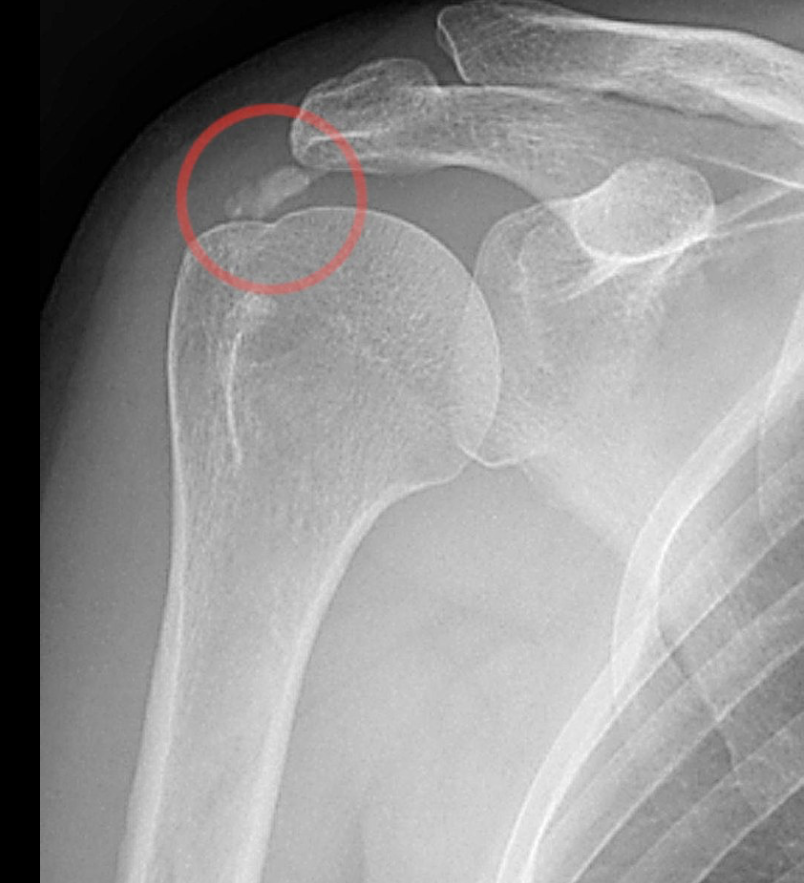
Xrays are the typical test of choice to see the calcification. The deposits look cloudy on X-ray if they are in the process of reabsorption, and this is also when they cause the most pain. The deposits are crystalline when in their resting phase and like toothpaste in the re-absorptive phase. Ultrasound is also useful to depict calcific deposits and closely correlates with the stage of disease.
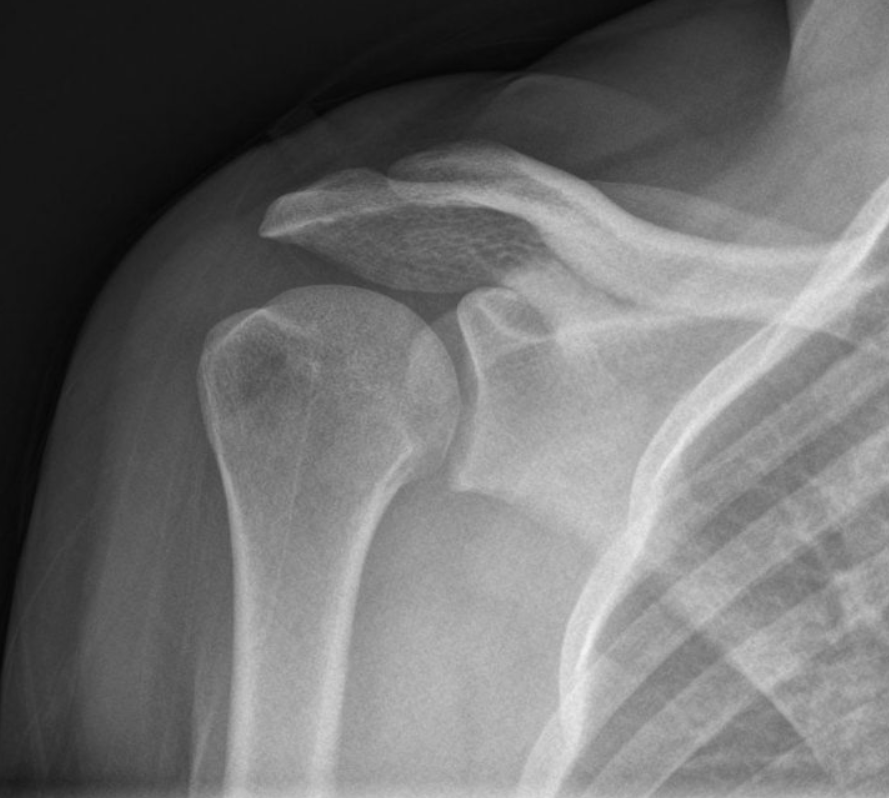
Normal Shoulder Xray
Abnormal Calcific Tendonitis Xrays
Treatments
There are many treatment options to help the patient suffering from calcific tendonitis and pain. Some of the initial treatment can include Physical therapy, oral anti-inflammatory medication, steroid injections, extracorporeal shock wave therapy, platelet-rich-plasma or stem cells have been shown to help.
When the patients fail to respond to these non-surgical non-invasive treatments, surgery can be considered to remove the calcium.
Another treatment that can be consider at this point is offer by Dr. Gonzalez, this is called Ultrasound Guided percutaneous barbotage calcium removal. This is a minimally invasive procedure performed in the office under local anesthesia where Dr. Gonzalez is able to find the calcium deposit with high-resolution ultrasound and remove it using a needle technique.